More than 5,000 scientists specializing in dementia met at the Alzheimer's Association International Conference (AAIC) July 18 to 23 in Washington D.C. to discuss the latest research on the cause, diagnosis, treatment and prevention of the disease.

Many eyes at the conference were on drug maker Eli Lilly's solanezumab, which may slow disease progression by about one-third, according to a new study. Other companies garnering attention for drugs in clinical trials were Roche for its gantenerumab and Biogen for its aducanumab. All of these drugs target beta amyloid, a complex protein that is often considered the culprit in forming the plaques that are characteristic of AD.
In an era of many aging baby boomers, a quarter of whom will get the disease - and a potential $10 billion market - everyone hopes that the latest clinical trial results will finally produce a promising treatment to slow or halt the progression of Alzheimer's disease (AD). In fact, by 2050, nearly 104 million people - or one-third of the American population - could have AD.
"Yet with lengthy timelines and many hurdles to overcome on the road to marketing approvals, a unique Tau-targeted approach could reach the finish line first," according to Professor Claude Wischik, co-founder and executive chairman of TauRx Therapeutics. While tangles of neuronal fibers caused by overproduction of Tau protein match up to abnormalities in brain scans of patients with AD, nobody has an approved treatment to target the tangles at the moment, Wischik says. His company's Phase III clinical trials of the Tau-aggregation inhibitor (TAI), LMTX, are fully recruited, with the first top-line results anticipated by Q2 2016, meaning that LMTX could be on the market as early as 2017.
Wischik has six papers to prove his point. Realizing the complicated nature of the subject and the need to present an unconventional view, he wanted to get as much information as he could out to the public in a short time. According to Wischik, the collection of papers "supports our central contention that abnormal aggregation of Tau protein is the main driver of clinical dementia, and that LMTX provides the first fully viable TAI as a novel basis for treatment and prevention of AD."
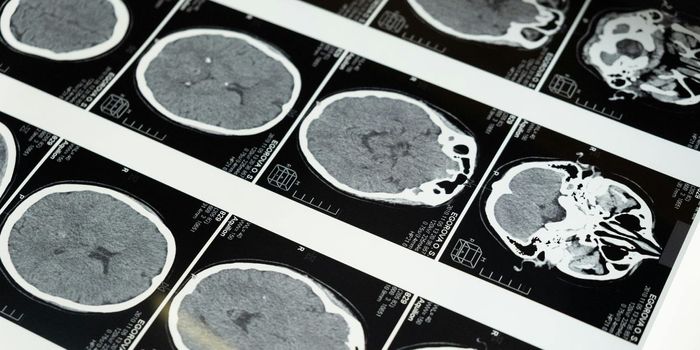
He added, "In three ongoing clinical trials involving 1,900 people, we have a reasonable sense that the drug is safe. A measuring scale of Amyloid Related Imaging Abnormalities (ARIA) showed that LMTX ranks below placebo studies on magnetic resonance imaging (MRI) tests.
"Analysts are having a problem finding a sweet spot between efficacy and ARIA," Wischik added. He believes that some people are still looking at amyloid therapy, because a large investment of time and money has gone in that direction. Potential AD treatments based on amyloid therapy that are in clinical trials appear to ease symptoms temporarily and have the potential for side effects, he said, while tau-based vaccines could be a more effective method of treating AD in the early stages of the disease
He explained that the first-generation TAI exhibited a 90-percent reduction in the rate of cognitive decline over 50 weeks in Phase II clinical trials. Also, an independent Mayo Clinic study of more than 3,600 post-mortem brains recently concluded that the progression of dysfunctional tau protein, not beta amyloid, drives the cognitive decline and memory loss seen in Alzheimer's disease.
"The imaging is completely objective," he said. "The treatment keeps areas of the brain from shutting down. Our drug acts on neurodegeneration, which can begin when people are in their 50s or 60s."
TauRx, a spinoff company from the University of Aberdeen, Scotland, was established in Singapore in 2002. Wischik and his colleagues at Aberdeen discovered that tangles were made up of abnormal filaments largely composed of a short fragment of the protein Tau in 1988. While the Phase II clinical trials were largely successful, they demonstrated reduced efficacy in the top dosage. TauRx scientists attributed the flaw to an absorption problem when LMTX is taken with food and developed a new form of the molecule that allows for enables direct absorption by the body.
One of the six papers explains the bioavailability problem and how it was solved with a chloride salt. It published the Phase 2 data in full as Wischik et.al., "Tau aggregation inhibitor therapy: an exploratory Phase 2 study in mold or moderate Alzheimer's disease," in the Journal of Alzheimer's Disease.
Another of the papers (Melis et.al, "Different pathways of molecular pathophysiology underlie cognitive and motor tauopathy phenotypes in two transgenic mouse tauopathy models, Behavioral Pharmacology) described two different Tau transgenic mouse models based on mutations in the Tau gene or Tau found in tangled filaments. As Wischik explained, "The Tau protein fragment functioned as a prion and replicateed itself. It produced symptoms in a motor domain of frontotemporal dementia. The model did not progess with age, but there was no cognitive impairment. The other model got progressively worse with age."
What the article proved is that there can be mouse dementia with no amyloid, according to Wischik. There are different pathways of molecular disease process with Tau, he explained. "The drug works in both models," he said. "It reduces Tau pathology and the effects of Tau pathology. They overlap at the minimum effective dose."
Other papers showed how the body processes the drug, described the efficacy of the dosage and showed what the drug looked like with X-ray crystallography. The final paper in the series showed the primary synthesis and characterization of the drug and the critical concentration required for breaking down Tau aggregates from brain tissue.
"We're delivering a broadside to the field of Alzheimer's disease research," Wischik concluded. "We're showing that we really know what this is about, that we're breaking ground and making new discoveries and leading the way at every step. We're preparing the ground for Phase 3 data and showing the fruits of what we've labored over many years to construct."